This is the sixth part of a blog about Robert Whitaker’s book, Anatomy of an Epidemic: Magic Bullets, Psychiatric Drugs and the Astonishing Rise of Mental Illness in America.
Okay… So this blog is about depression. And, of course, those “magic bullets,” the anti-depressants.
Some background: Community surveys from the 1930’s and 1940’s found fewer than one in a thousand people suffered an episode of clinical depression each year. And most of those who did, did not require hospitalization. In 1955, the disability rate from depression was one in 4,345 people. Oh, and it was a disease of the middle-aged and the elderly. Hold that thought.
Study after study from these years showed that folks with depression had great prospects for recovery via spontaneous remission… about half, in fact. And folks recovering from depressive episodes had the same “capacity and prospects” in their work life as before the onset of the illness. In other words, they were not being disabled by depression.
Okay… So this blog is about depression. And, of course, those “magic bullets,” the anti-depressants.
Some background: Community surveys from the 1930’s and 1940’s found fewer than one in a thousand people suffered an episode of clinical depression each year. And most of those who did, did not require hospitalization. In 1955, the disability rate from depression was one in 4,345 people. Oh, and it was a disease of the middle-aged and the elderly. Hold that thought.
Study after study from these years showed that folks with depression had great prospects for recovery via spontaneous remission… about half, in fact. And folks recovering from depressive episodes had the same “capacity and prospects” in their work life as before the onset of the illness. In other words, they were not being disabled by depression.

The first generation of anti-depressants got good press... for a while. But then the National Institute of Mental Health noted that the more rigorous the controls for studies, the lower the improvement rates. Turns out that placebos were just as effective.
And then, in 1988, Prozac hit the market with a splash of publicity... for a while. It turned out that the SSRI’s (selective serotonin reuptake inhibitors) were no better than the earlier generation of anti-depressants when compared with placebos.
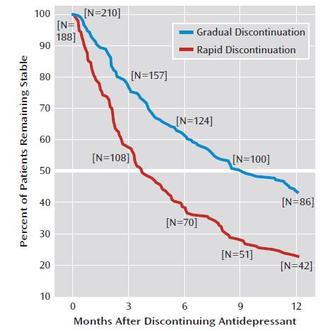
But there was one area where anti-depressants were having a definite effect.... Patients on long-term anti-depressant use were experiencing depression as a chronic condition. Not only that, but a chronic condition they were stuck with, because when the patients tried to get off their meds, they would have hideous relapses of clinical depression, often accompanied by suicidal ideation. Researchers referred to it as “rapid clinical deterioration.” And the longer the course of medication, the more serious the relapse.
And then, in 1988, Prozac hit the market with a splash of publicity... for a while. It turned out that the SSRI’s (selective serotonin reuptake inhibitors) were no better than the earlier generation of anti-depressants when compared with placebos.
But there was one area where anti-depressants were having a definite effect.... Patients on long-term anti-depressant use were experiencing depression as a chronic condition. Not only that, but a chronic condition they were stuck with, because when the patients tried to get off their meds, they would have hideous relapses of clinical depression, often accompanied by suicidal ideation. Researchers referred to it as “rapid clinical deterioration.” And the longer the course of medication, the more serious the relapse.
Yep… the anti-depressants were joining the neuroleptics and the benzodiazepines as psychiatric drugs proving to cause more serious conditions than those they purported to cure. And pretty much for the same reason: The drugs were introducing a chemical imbalance to the brain, and the brain was making drastic adjustments to compensate. These adjustments, over time, would become permanent, which is why withdrawal of the drugs had such disastrous consequences. The brain had now become permanently imbalanced.
But the investment in these "magic bullets" was enormous. In response to the evidence of harm, the medical establishment began to circle their theory wagons. They found a way to explain away the earlier, pre-1960 history of depression: Apparently, the reason so many depressed patients seemed to recover so easily in the past was because the doctors back then had inferior systems for describing and classifying mental illness. Depression, they insisted, is, and always has been, a chronic condition requiring medication... and any statistics that would contradict this must be invalid. Why, all you had to do was look at how many patients relapsed when they went off their meds, to see how necessary the drugs are!
So let me recap: Prior to the discovery of anti-depressants, depression was reported as relatively rare, and with good prospects of complete recovery. Children and young people hardly ever suffered from it. Today, one in ten people are diagnosed with depression as a chronic condition, and these folks can expect recurrences throughout their lives. In fact, two-thirds of patients treated with anti-depressants can expect recurrent bouts. In one study, only 6% could expect remission.
In a 1995 study by the NIMH, patients who had been medicated for depression were likely to have become disabled. And children and young people? Today depression is the leading cause of disability for folks between the ages of 15 and 44.
And then, of course, there are the side effects: The SSRI’s can cause sexual dysfunction, suppression of REM sleep (which will cause psychiatric problems), fatigue, emotional blunting, and apathy. And… impaired memory, impaired problem-solving ability, loss of creativity, learning disabilities. All this for a short-term effect often little better than that of a placebo, likely to result in chronic depression, with possible disability. Such a deal.
But the investment in these "magic bullets" was enormous. In response to the evidence of harm, the medical establishment began to circle their theory wagons. They found a way to explain away the earlier, pre-1960 history of depression: Apparently, the reason so many depressed patients seemed to recover so easily in the past was because the doctors back then had inferior systems for describing and classifying mental illness. Depression, they insisted, is, and always has been, a chronic condition requiring medication... and any statistics that would contradict this must be invalid. Why, all you had to do was look at how many patients relapsed when they went off their meds, to see how necessary the drugs are!
So let me recap: Prior to the discovery of anti-depressants, depression was reported as relatively rare, and with good prospects of complete recovery. Children and young people hardly ever suffered from it. Today, one in ten people are diagnosed with depression as a chronic condition, and these folks can expect recurrences throughout their lives. In fact, two-thirds of patients treated with anti-depressants can expect recurrent bouts. In one study, only 6% could expect remission.
In a 1995 study by the NIMH, patients who had been medicated for depression were likely to have become disabled. And children and young people? Today depression is the leading cause of disability for folks between the ages of 15 and 44.
And then, of course, there are the side effects: The SSRI’s can cause sexual dysfunction, suppression of REM sleep (which will cause psychiatric problems), fatigue, emotional blunting, and apathy. And… impaired memory, impaired problem-solving ability, loss of creativity, learning disabilities. All this for a short-term effect often little better than that of a placebo, likely to result in chronic depression, with possible disability. Such a deal.

And here I am departing from a review of Whitaker’s book to take a sidetrip to a website called SSRI Stories. This is not for the faint-of-heart: Here's their self-description: "This website is a collection of 4,300+ news stories with the full media article available, mainly criminal in nature, that have appeared in the media (newspapers, TV, scientific journals) or that were part of FDA testimony in either 1991, 2004 or 2006, in which antidepressants are mentioned."
And the stories are doozies. For the reader's convenience, the website has categorized them by atrocity. Here's the list:
Soldier Cases
School Shootings / Incidents
Most Recent (Last 30 Days)
Workplace Violence
Celebrity Cases
Highly Publicized Cases
Won SSRI Criminal Cases
Women Teacher Molestations
Postpartum Cases
Murder-Suicides
Murders / Murder Attempts
Suicides / Suicide Attempts
Road Rage Cases
If you click on any of these, you can read the details about these cases, with links to corresponding journal or newspaper articles. Is the association with anti-depressants a coincidence? I mean, only people with depression and mental illness are prescribed the drugs, so is it fair to blame these crimes on pharmaceuticals? Check out the narratives from family members, insisting that, prior to the use of medications, the person did not have suicidal ideation, mood swings, erratic behavior. Check out how many times drug companies have paid out claims on these cases... and you know that these settlements are not cheap.
Finally, the FDA has had to admit that the SSRI's are causing children and young people to take their lives, and labels now have to carry warnings about increased risk of suicide among young adults aged 18 to 24. Clearly, the folks who run the SSRI Stories website see this as just the tip of the iceberg, and, at least to me, they make a compelling case.
So, since the anti-depressants have such poor efficacy and such gargantuan risks, why are so many people still taking them? In the US, by 2005, one in ten people were on anti-depressants. By 2008, there were 164 million prescriptions written for anti-depressants.
What the hell is going on? Stay tuned!
Click here to go back to Part 1.
Click here to go on to Part 7.
And the stories are doozies. For the reader's convenience, the website has categorized them by atrocity. Here's the list:
Soldier Cases
School Shootings / Incidents
Most Recent (Last 30 Days)
Workplace Violence
Celebrity Cases
Highly Publicized Cases
Won SSRI Criminal Cases
Women Teacher Molestations
Postpartum Cases
Murder-Suicides
Murders / Murder Attempts
Suicides / Suicide Attempts
Road Rage Cases
If you click on any of these, you can read the details about these cases, with links to corresponding journal or newspaper articles. Is the association with anti-depressants a coincidence? I mean, only people with depression and mental illness are prescribed the drugs, so is it fair to blame these crimes on pharmaceuticals? Check out the narratives from family members, insisting that, prior to the use of medications, the person did not have suicidal ideation, mood swings, erratic behavior. Check out how many times drug companies have paid out claims on these cases... and you know that these settlements are not cheap.
Finally, the FDA has had to admit that the SSRI's are causing children and young people to take their lives, and labels now have to carry warnings about increased risk of suicide among young adults aged 18 to 24. Clearly, the folks who run the SSRI Stories website see this as just the tip of the iceberg, and, at least to me, they make a compelling case.
So, since the anti-depressants have such poor efficacy and such gargantuan risks, why are so many people still taking them? In the US, by 2005, one in ten people were on anti-depressants. By 2008, there were 164 million prescriptions written for anti-depressants.
What the hell is going on? Stay tuned!
Click here to go back to Part 1.
Click here to go on to Part 7.